Dear Brothers,
As the year comes to an end and we look toward new beginnings, this message is for my fellow Black queer men—especially those of us navigating late-night party culture. This piece addresses the complex and occasionally risky dynamics of chemsex spaces, including the practices known as PnP (party and play) and HnH (high and horny).
I write this, not as a lecture, but as a gentle letter composed with care, honesty, and a commitment to our collective survival and Black joy. As Black queer men, we carry heavy burdens that you really have to be one of us to understand. Even from a scientific perspective, being Black and queer means we face compounded minority stress due to intersecting pressures.
There’s no shame in looking for relief, connection, pleasure, or escape in these spaces. Wanting to feel good is not weakness — it’s survival. But instead of dwelling on systems that consistently fail to prioritise us, let’s focus on forging new paths that better serve our needs.
Why Black Queer Men Turn To Chemsex
Many Black queer men often turn to substance use as a way of coping with a unique combination of stressors. Researchers consistently note that minority stress—the chronic strain from stigma, discrimination, and social exclusion faced by marginalised individuals—significantly increases vulnerability to anxiety, depression, and other mental health issues (Meyer, 20036; Schuler et al., 2020)8.
Statistics confirm this:
Large-scale U.S. data show that sexual minority adults, including Black gay and bi men, are significantly more likely to use illicit substances than heterosexual adults. Approximately 37% of sexual minority adults reported past-year illicit drug use, compared to 17% of heterosexual adults (Rosner et al., 2021)7.
The HIV Disparity
Researchers and analysts note that systemic barriers, rather than inherently riskier behaviour, drive the disproportionate HIV burden among Black gay and bisexual men. In 2024, CDC data showed Black gay and bisexual men accounted for 26% of new HIV diagnoses among men who have sex with men (MSM), despite representing a much smaller share of the population (CDC, 2024)2.
Other Aggravating Issues
For Black queer men, stressors are intensified by:
- Exclusion and under-representation in some queer spaces.
- Increased exposure to microaggressions and shaming.
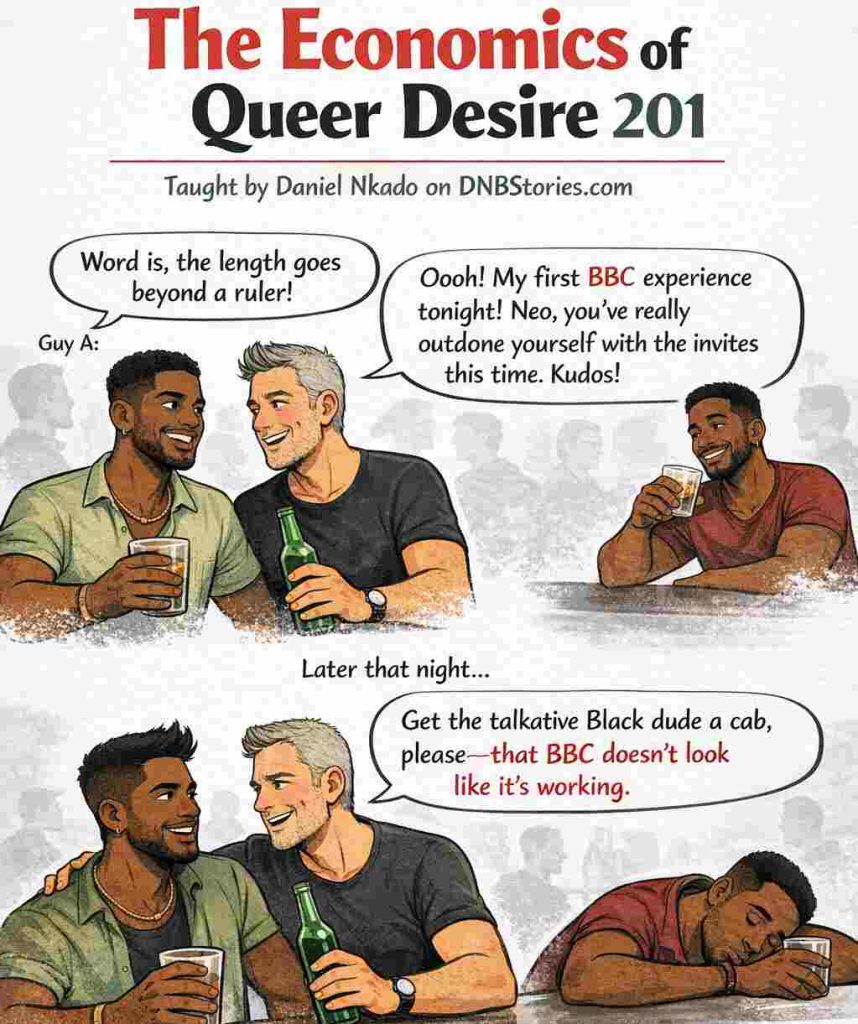
- Fetishisation and being treated as a fantasy rather than a full person (e.g., “BBC” stereotypes).
- Feeling “too Black” in white queer spaces and “too queer” in Black spaces. Constant worry about feeling “out of place” creates distress and may ultimately lead to isolation.
- Violence and criminalisation create extra problems for Black queer men living in hostile countries.
We are not weak for seeking ways to forget trauma. None of us planned to be born in a world that makes everything so exhausting. But we at least owe it to ourselves to be honest and take care of ourselves and each other.
The Specific Reality of Chemsex for Black Queer Men
Chemsex typically involves drugs such as crystal methamphetamine (“Tina” or “T-Drug”), mephedrone, and GHB/GBL (“G”) to enhance or prolong sexual encounters. While these substances may temporarily increase confidence or euphoria, chemsex environments can be uniquely hostile and risky for Black men.
The Hidden Risks in Chemsex Spaces
- Fetishisation: Many Black men report degrading comments, being subjected to racialised fantasies, or pressure to perform.
- Consent challenges: High intoxication makes it difficult to establish or maintain consent, increasing vulnerability to sexual risk and assault (Bourne et al., 2015)1.
- Dehumanisation: In some predominantly White chemsex scenes, Black gay men may experience both fetishisation (“I’ve always wanted to try a Black guy”) and humiliation (“Get the sleepy Black guy a cab—that dick is not working”), sometimes in the same night.
Current Risks Readers Should Know About
1. The Fentanyl Crisis
Drug supplies can be unstable, and in some regions, fentanyl contamination has been found in non-opioid drugs. The level of risk varies by place, so readers should check current local alerts and carry naloxone where opioid contamination is a possibility.
Fentanyl’s high potency means a minuscule amount can be lethal. It poses a high risk for fatal overdose, especially for unsuspecting users.
In some settings, fear of police contact, criminalisation, shame, or exposure can delay emergency calls during overdoses, which increases danger (Johnson et al., 2022)5.

2. GHB/GBL (‘G’) and the ‘Drop’
GHB is a depressant with a steep dose–response curve, meaning the gap between a “fun” dose and a dangerous one is very small. The difference between euphoria and unconsciousness can be as little as 1 millilitre.
- Danger: Rapid sedation increases vulnerability to sexual assault.
- Physiology: Mixing G with alcohol or other depressants significantly increases the risk of respiratory failure (Tay et al., 2022)9.
With GHB/GBL:
- Avoid GHB/GBL + alcohol + benzodiazepines (like Xanax or Valium). This is a high-risk combo for overdose and respiratory arrest.
- Because GHB has a narrow safety window, even experienced users can accidentally overdose.
- Use a measured syringe or dropper, not “just a cap.”
- Set a timer (e.g., 2–3 hours) before even considering a redose.
- If someone looks unresponsive, call emergency services immediately—do not just “let them sleep it off” (Freestone et al., 2023)4.
- In the UK, call 999 in an emergency. If you want non-judgmental support around chemsex, speak to your local sexual health clinic or specialist services such as AXIS Clinic or Club Drug Clinic if you are in their areas.
If you are unsure whether someone needs help, always call emergency services—breathing problems can escalate quickly.
3. Crystal Meth and the ‘Crash’
Methamphetamine causes a surge of dopamine, followed by a severe crash or comedown. A meth comedown can leave users feeling unhappy, anxious, or agitated. Intense depression, paranoia, and psychosis can occur after prolonged use or lack of sleep.
Long-term meth use can alter brain structures involved in reward and emotion, making it harder to feel pleasure without the drug (Thompson et al., 2004)10.
A study involving gay men who engage in chemsex in South London shows that poor knowledge of dosing—especially with GHB/GBL—led to frequent overdoses and “near misses,” and many men often struggled with consent, anxiety, and low mood afterwards, yet avoided traditional drug services, due to fear of judgment and cultural misunderstanding (Bourne et al., 2015)1.
8 Harm Reduction Strategies for Black Queer Men
This is not a call for abstinence. It is a toolkit for survival, autonomy, and care.
1. Check in With Yourself
“Checking in with yourself” means pausing whatever you’re doing and using mindfulness and honest reflection to assess what’s happening in your body, mind, and emotions in the present moment.
Before opening an app or heading to a party, ask:
- What do I need tonight—sex, validation, escape, connection?
- Am I grounded enough to make decisions that protect me?
Understanding your need helps you stay in control and align your actions more effectively with your goal.
2. Vet the Space
- Read the room: How are Black men being spoken to in group chats or messages?
- Trust your gut: If the energy feels racist, coercive, predatory, or unsafe, do not go. Power imbalances increase risk.
3. Set Non-Negotiable Boundaries
Decide your limits while sober and stick to them. You can write them out and share with the host before taking any drug.
- “No injection.”
- “I only take G if I measure it myself.”
- “No trying of any new substance I haven’t done before.”
- “I will stop at 1 AM, no matter how I am feeling.”
4. Use the ‘Lifeline’ Protocol
This is exceptionally important for Black queer men living in more dangerous cities.
- Tell a trusted friend where you’re going.
- Share your live location.
- Set a check-in time and a safe word or emoji.
- Permit them to intervene if you go silent.
5. Carry Your Personal Harm Reduction Toolkit
- Fentanyl test strips: You can often get them from online pharmacies, harm-reduction services, or platforms like Amazon, depending on your country.
- Naloxone (Narcan): It reverses opioid overdose, but not GHB/GBL or meth overdose on its own.
- Condoms, PrEP, and U=U-aware partners: Prevention is power.
- PEP access: Know where to go within 72 hours to get PEP if needed.
- Get regular HIV, STI, and hepatitis C testing, and ensure your hepatitis A and B vaccinations are up to date.
6. Start Low, Go Slow
- Time your G: Use a timer. Never redose within 2–3 hours.
- Measure properly: Use a syringe, never a bottle cap.
- Never redose if you can’t remember when or how much you last took — when in doubt, wait it out.
- Understand that injecting carries significant risks: These include injury, infection, blood-borne viruses, and a higher risk of overdose.
If you inject, please use sterile equipment every time and never share needles, barrels, water, or other injecting equipment. If you want help reducing injecting-related risks, speak to a specialist sexual health or drug service. Non-injecting routes may avoid needle-related harms, but they still carry serious risks and are not ‘safe’.
7. Know the Recovery Position
If someone is unconscious but breathing:
- Roll them onto their side.
- Tilt their head back to open the airway.
- Call for help if breathing slows or stops.
8. Plan Your Aftercare
The days after a session can be emotionally fragile.
- Prepare food and electrolytes.
- Prioritise sleep.
- Reach out to community advocates if depression intensifies.
- Consider having a trusted brother or queer-friendly therapist lined up for any unforeseen events. Local Black LGBTQ organisations have peer support groups that understand chemsex and provide care without shaming.
A Word To Other Black Men
Please take care of each other!
In high-risk chemsex and PnP spaces, safety depends on mutual care. Historically, we have always protected each other even when the world wouldn’t. Looking out for one another can be simple: checking in, ensuring safe travel, intervening when the energy shifts, or challenging acts of racism, fetishisation, pressure, shaming and disrespect.
And most importantly, never allowing yourself to become an instrument of harm to another brother. This is the unspoken code we shared where I grew up. It is sacred. Our well-being is interconnected. Supporting one another strengthens us all.
One risky night does not define your worth, your masculinity, or your capacity to heal and grow. Let’s look out for each other in 2026.
With love,
Daniel.
References
- Bourne, A., Reid, D., Hickson, F., Torres-Rueda, S., & Weatherburn, P. (2015). “Chemsex” and harm reduction needs among gay men in South London. International Journal of Drug Policy, 26(12), 1171–1176. https://doi.org/10.1016/j.drugpo.2015.07.013
- Centres for Disease Control and Prevention. (2024, October 7). Fast facts: HIV and gay and bisexual men. https://www.cdc.gov/hiv/data-research/facts-stats/gay-bisexual-men.html
- Drug Enforcement Administration — DEA. (n.d.). Facts about fentanyl. https://www.dea.gov/resources/facts-about-fentanyl
- Freestone, J., Ezard, N., Bourne, A., Brett, J., Roberts, D. M., Hammoud, M., Nedanoski, A., Prestage, G., & Siefried, K. J. (2023). Understandings, attitudes, practices and responses to GHB overdose among GHB consumers. Harm Reduction Journal, 20(1). https://doi.org/10.1186/s12954-023-00857-z
- Johnson, L. M., Devereux, P. G., & Wagner, K. D. (2022). The group-based law enforcement mistrust scale: psychometric properties of an adapted scale and implications for public health and harm reduction research. Harm Reduction Journal, 19(1). https://doi.org/10.1186/s12954-022-00635-3
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
- Rosner, B., Neicun, J., Yang, J. C., & Roman-Urrestarazu, A. (2021). Substance use among sexual marginalised groups in the US—Linked to inequalities and unmet need for mental health treatment? Journal of Psychiatric Research, 135, 107–118. https://doi.org/10.1016/j.jpsychires.2020.12.023
- Schuler, M. S., Prince, D. M., Breslau, J., & Collins, R. L. (2020). Substance Use Disparities at the Intersection of Sexual Identity and Race/Ethnicity: Results from the 2015–2018 National Survey on Drug Use and Health. LGBT Health, 7(6). https://doi.org/10.1089/lgbt.2019.0352
- Tay, E., Lo, W. K. W., & Murnion, B. (2022). Current insights on the impact of gamma-hydroxybutyrate (GHB) abuse. Substance Abuse and Rehabilitation, 13, 13–23. https://doi.org/10.2147/SAR.S315720
- Thompson, P. M., Hayashi, K. M., Simon, S. L., Geaga, J. A., Hong, M. S., Sui, Y., Lee, J. Y., Toga, A. W., Ling, W., & London, E. D. (2004). Structural abnormalities in the brains of human subjects who use methamphetamine. The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, 24(26), 6028–6036. https://doi.org/10.1523/JNEUROSCI.0713-04.2004



How can I donate?